

Translational Science Benefits




Summary
When the spread of COVID-19 led to school closures, there were concerns about the broad effects that closures could have on the health and well-being of children and families.1 There were also questions about what strategies could be reliably implemented in a school setting to prevent the spread of COVID-19, including when vaccines would become available and how they would be received by youth and parents.2,3 While early research pointed to seemingly milder symptoms in most children and adolescents,4–6 schools that were early to reopen experienced outbreaks forcing additional closures.7,8 As private schools, and later public schools, in Orange County, California, sought to bring students back in person safely, schools and districts needed research-based guidance and feasible strategies to help navigate the novel coronavirus and changing public health guidelines.

In 2020, Orange County Healthy Schools Restart Group (OCHSRG) was formed to support schools and districts as they navigated operations during the COVID-19 pandemic. The group consists of virologists, pediatricians, educators, biologists, infectious disease specialists, psychologists, nurses, epidemiologists, and public health experts spanning numerous organizations in the region including the University of California, Irvine, Children’s Hospital Orange County, Orange County Health Care Agency, American Academy of Pediatrics Chapter 4, and the Orange County Department of Education.
When the group was initially formed, it was unknown what support schools would need and what role the group would play. As the pandemic progressed, the group provided numerous forms of vital support for school reopening, including research-based guidance on developing safe reopening plans for schools, interpretation of changing guidelines published by the Centers for Disease Control and Prevention (CDC), state, and county health departments, and updated resources that enabled schools to minimize exposures to COVID-19 based on current health guidelines.9 Group members also conducted their own research to contribute to the understanding of the coronavirus and the role schools play in its transmission and mitigation.1,10–12
Following schools reopening, the group developed resources to support the safe return to schools. These resources included 1) a Student Symptom Decision Tree, developed in collaboration with the Orange County Health Care Agency, that conveys changing public health guidelines for working with individuals with COVID-19 or exposure to COVID-19, 2) the Systematic Observation of COVID-19 Mitigation (SOCOM), developed in collaboration with researchers at Northern Arizona University, a protocol for assessing adherence to disease mitigation strategies, and 3) health education resources for physicians, educators, and parents.
Significance
OCHSRG demonstrated that a multidisciplinary collaboration of academic, public health, and education professionals is a successful approach to address the changing and multifaceted needs of school communities during the COVID-19 pandemic. Building on relationships with local private schools, the group reviewed 25 school waivers outlining COVID-19 protocols for in-person instruction in order to strengthen the reopening plans and minimize risk to students, faculty, and staff. The group also created resources and protocols that could be used as a model for effectively communicating public health guidance for COVID-19 and other diseases.10 Additionally, group members became involved in state and local committees to inform mask, vaccination, and ongoing return-to-school policies throughout the state.
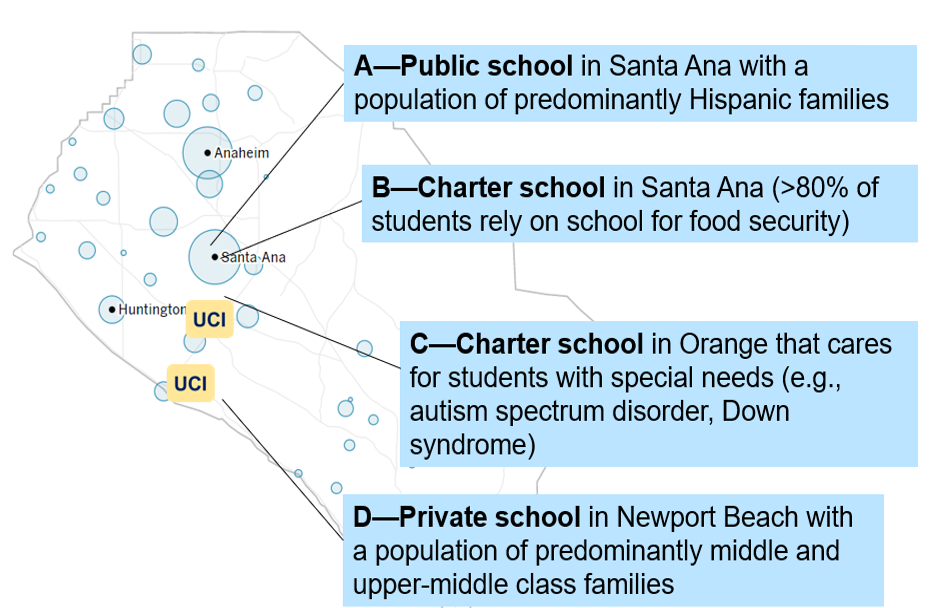
To promote equity and ensure representation when conducting research in schools, sites were chosen to represent the diverse Orange County student populations, as shown below. Sites selected included a school serving historically underserved populations and a school serving large numbers of children with special needs, a population for whom social distancing is more difficult to implement. Blood tests at these four schools indicated that case rates for schools closely reflected the larger community case rates.11 The group also revealed wide-ranging adherence to distancing and masking efforts in schools, including in special education classes.11
Benefits
Demonstrated benefits are those that have been observed and are verifiable.
Potential benefits are those logically expected with moderate to high confidence.
Clinical & medical benefits
The group, in conjunction with the Orange County Health Care Agency, developed Student and Staff Symptom Decision Trees that were distributed by the Orange County Department of Education to schools throughout Orange County to convey up to date guidelines for working with individuals with symptoms or exposure to COVID-19. demonstrated.
Developed a systematic observation protocol to capture adherence to COVID-19 mitigation strategies in school environments, known as the Systematic Observation of COVID-19 Mitigation (SOCOM).12 demonstrated.
Community & public health benefits
Provided talking points to nurses staffing the Children’s Hospital Orange County COVID-19 Hotline to reduce inconsistent responses to calls. demonstrated.
Created and disseminated health education resources such as FAQs on masking, vaccines, and other COVID-19 topics to school personnel, families, local nurses, and physicians. demonstrated.
Advised 25 schools on their Safe Reopening Plans and provided Decision Trees to help school nurses with decision making for potential COVID-19 cases and reduce disease spread. potential.
Use of the Student and Staff Symptom Decision Trees at schools is likely to improve life expectancy and quality of life by preventing further spread and reducing the incidence of hospitalization and death due to COVID-19. potential.
Economic benefits
The group’s efforts to limit the spread of COVID-19 in schools allowed students to return to school without increasing case rates of COVID-19. potential.
Policy & legislative benefits
Members of the group participated in the Orange County Health Care Agency Vaccine Task Force to provide guidance for Orange County on vaccine distribution, and one group member participated in the California Vaccine Coalition. demonstrated.
A group member served as an expert witness for the state of California in a lawsuit that upheld the California mask mandate.13 demonstrated.
This research has clinical, community, economic, and policy implications. The framework for these implications was derived from the Translational Science Benefits Model created by the Institute of Clinical & Translational Sciences at Washington University in St. Louis.14
Clinical
The Orange County Healthy Schools Restart Group (OCHSRG) measured adherence to COVID-19 mitigation strategies within a variety of school settings by developing a new investigative tool with researchers at Northern Arizona University, the Systematic Observation of COVID-19 Mitigation (SOCOM).12 The tool allowed observers to track mitigation adherence in a paper or electronic form. This investigative procedure can easily be used in a variety of settings to evaluate the consistency of following public health guidelines. Data showed that mitigation procedures can be widely followed in a school environment.12 The OCHSRG, in conjunction with the Orange County Health Care Agency, also developed Student and Staff Symptom Decision Trees that were available during the 2021-2022 school year for use by all 600 K-12 schools in Orange County.9 The decision trees were used to effectively convey changing public health guidelines and steps to take for people with possible COVID-19 exposure to increase the safety of others at the school site.
Community
The group created multiple health education resources to communicate scientific guidelines and information about COVID-19 to the broader community. In August 2021, the group disseminated a letter on the importance of face coverings along with the Student Symptom Decision Tree to families of students within all 600 K-12 schools in Orange County.15 This letter focused on explaining the science of viruses, the role masks play in preventing disease, and how to use the decision tree.15 The group also created and disseminated multiple FAQ documents for school nurses, school administrators, and parents. Group members also organized and participated in COVID-19 webinars, including 4 webinars focused specifically on educating and fielding questions from school nurses. Additionally, the group collaborated with Children’s Hospital Orange County to evaluate the questions being answered by a COVID-19 hotline. This evaluation revealed common questions and inconsistencies in the responses given, which led to creating a document of the top 10 FAQs and providing talking points for the hotline staff to reduce inconsistencies in the information provided during calls, increasing the quality of care.
The group also reviewed school reopening plans to enhance mitigation procedures and responses to COVID-19 exposures and cases within the school. They reviewed 25 schools’ plans and offered recommendations on topics that included screening procedures, isolation rooms, illness management, shared spaces, and monitoring the efficacy of the reopening plan. The group’s focus on safe reopening helped to prevent the spread of COVID-19 in the school setting.
Economic
The group’s attention to factors that limit the spread of COVID-19 in schools allowed students to return to school without increasing case rates of COVID-19 and enabled parents in Orange County to return to work, likely reducing the societal and financial cost of COVID-19.
Policy
Multiple group members participated in the Orange County Health Care Agency Vaccine Task Force, which provided guidance for Orange County vaccine distribution. One group member also participated in the California-wide committee that advised the state’s vaccine roll-out, reporting directly to the Lieutenant Governor. Another group member served as an expert witness on the efficacy of masking for the State of California in the lawsuit attempting to overturn the California mask mandate in schools, with the court ruling that the mask mandate was lawful and could remain in place.13
Lessons Learned
Relationships were critical to the success of the group, including the established relationships that individual members had across health organizations in the county and within local schools. These existing relationships allowed the group to determine what the needs of schools and constraints on their staff were and leverage this knowledge to assist other schools in the area.
The group included virologists, pediatricians, educators, biologists, infectious disease specialists, psychologists, nurses, epidemiologists, and public health experts. The group members’ multi-disciplinary expertise was essential to address the complexity of the situation. The collaboration of a diverse set of professionals allowed for interpretation of policies into practical implementation strategies and enabled broad availability of guidance within Orange County schools.
Funding: This work was funded through the Clinical and Translational Science Awards from the National Center for Advancing Translational Sciences, NIH (UL1 TR001414, R01AI142841, R21AI143301) the University of California Irvine’s COVID-19 Basic, Translational and Clinical Research Fund, and the Northern Arizona University Southwest Health Equity Research Collaborative (NIH/NIMHD U54; U54MD012388). Support was provided in part by the Robert Wood Johnson Foundation, the National Institute of Allergy and Infectious Diseases, NIH (K08 AI151253-01), the National Institutes of Health Community Engagement Alliance against COVID-19 Disparities award (21-312-0217571-66106L, 21-312-0217571-66106), and the Orange County Health Care Agency Research Fund.
- Cooper DM, Guay-Woodford L, Blazar BR, et al. Reopening Schools Safely: The Case for Collaboration, Constructive Disruption of Pre-Coronavirus 2019 Expectations, and Creative Solutions. The Journal of Pediatrics. 2020;223:183-185. doi:10.1016/j.jpeds.2020.05.022
- Cooper DM, Afghani B, Byington CL, et al. SARS-CoV-2 vaccine testing and trials in the pediatric population: biologic, ethical, research, and implementation challenges. Pediatr Res. 2021;90(5):966-970. doi:10.1038/s41390-021-01402-z
- Hopfer S, Fields EJ, Ramirez M, et al. Adolescent COVID-19 Vaccine Decision-Making among Parents in Southern California. IJERPH. 2022;19(7):4212. doi:10.3390/ijerph19074212
- Yasuhara J, Kuno T, Takagi H, Sumitomo N. Clinical characteristics of COVID‐19 in children: A systematic review. Pediatric Pulmonology. 2020;55(10):2565-2575. doi:10.1002/ppul.24991
- Mehta NS, Mytton OT, Mullins EWS, et al. SARS-CoV-2 (COVID-19): What Do We Know About Children? A Systematic Review. Clinical Infectious Diseases. 2020;71(9):2469-2479. doi:10.1093/cid/ciaa556
- Bhuiyan MU, Stiboy E, Hassan MdZ, et al. Epidemiology of COVID-19 infection in young children under five years: A systematic review and meta-analysis. Vaccine. 2021;39(4):667-677. doi:10.1016/j.vaccine.2020.11.078
- Stein-Zamir C, Abramson N, Shoob H, et al. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Eurosurveillance. 2020;25(29). doi:10.2807/1560-7917.ES.2020.25.29.2001352
- Otte im Kampe E, Lehfeld AS, Buda S, Buchholz U, Haas W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Eurosurveillance. 2020;25(38). doi:10.2807/1560-7917.ES.2020.25.38.2001645
- Healthy School Restart Working Group Hub. UC Irvine Institute for Clinical and Translational Science. Accessed December 16, 2022.
- Salazar Campo M, Miovsky N, Schneider M, et al. Formative Evaluation of a Student Symptom Decision Tree for COVID-19. Health Behav Policy Rev. 2023;10(1):1140-1152. doi:10.14485/HBPR.10.1.1
- Cooper DM, Zulu MZ, Jankeel A, et al. SARS-CoV-2 acquisition and immune pathogenesis among school-aged learners in four diverse schools. Pediatr Res. 2021;90(5):1073-1080. doi:10.1038/s41390-021-01660-x
- Camplain R, Lopez NV, Cooper DM, McKenzie TL, Zheng K, Radom-Aizik S. Development of the systematic observation of COVID-19 mitigation (SOCOM): Assessing face covering and distancing in schools. J Clin Trans Sci. 2021;5(1):e124. doi:10.1017/cts.2021.786
- Taketa K. Judge dismisses lawsuit challenging Newsom’s school mask rules. Los Angeles Times. Published November 13, 2021. Accessed December 21, 2022.
- Institute of Clinical & Translational Sciences at Washington University in St. Louis. Translational Science Benefits Model website. Published February 1, 2019.
- Institute for Clinical and Translational Research. Healthy School Restart Working Group Hub. Memo: The Importance of Vaccines and Mask Wearing. Accessed January 4, 2023.